
{kind=link}
I’ve written about the Vaccine Adverse Events Reporting System (VAERS) database many times, particularly how antivaxxers have weaponized its contents to falsely portray COVID-19 vaccines as deadly and, before the pandemic, to falsely link childhood vaccines with autism, infertility and premature ovarian insufficiency, sudden infant death syndrome (SIDS), and more. It is a longstanding strategy that has been used by the antivaccine movement going back at least two decades. The reason for this is simple. As a passive reporting system into which anyone can enter any adverse event after vaccination (e.g., that a vaccine turned one into the Incredible Hulk), VAERS was never intended to provide an epidemiologically reliable estimate of the frequency of specific adverse reactions to vaccines. Rather it was intended to be a “canary in the coalmine”, a hypothesis-generating system in which increased reports of specific adverse events can raise safety signals that generate hypotheses. These hypotheses are then tested in more rigorous active reporting systems, such as the Vaccine Safety Datalink. Because of its nature, VAERS is subject to serious reporting bias, both under- and over-reporting depending on the specifics, and antivaxxers who incompetently analyze its contents (including sometimes even those who aren’t antivaccine) often fail to consider the underlying baseline rate of the various adverse events in the database. For example, the number of deaths reported after COVID-19 vaccination might seem alarmingly large until one takes into account how many people in the US die each and every day (over 3 million/year, or over 8,000/day), vaccination or no vaccination and estimates how many people would be expected to die sometime soon after a COVID-19 vaccination by random chance alone, particularly taking into account the various age groups.
Given that the shortcomings of VAERS are now much more widely known, I was wondering when the antivaccine movement would try to dumpster dive in a different health database to demonize COVID-19 vaccines. Just such an effort has started going viral on social media as a result of Sen. Ron Johnson’s (R-Wisc) “COVID-19: A Second Opinion” discussion panel, held the day after the antivaccine “Defeat the Mandates” rally in Washington, DC two weeks ago and featuring a rogues’ gallery of COVID-19 contrarians, cranks, minimizers, and antivaxxers promoting misinformation. During the panel, Ohio attorney Thomas Renz, a man associated with the COVID-19 misinformation group America’s Frontline Doctors and known for spreading antivaccine misinformation before the pandemic (e.g., among the orthodox Jewish community in New York) testified that there has been a dramatic three-fold increase in cancer among military personnel since the COVID-19 vaccines rolled out, citing three Department of Defense (DoD) “whistleblowers” that he represents, Drs. Samuel Sigoloff, Peter Chambers, and Theresa Long, who downloaded what’s characterized as a “massive trove of unclassified data” from the Defense Medical Epidemiology Database (DMED) and provided it in an Excel spreadsheet (because that’s how we love to analyze complex epidemiological data). This was not the only adverse event that the “whistleblowers” claimed to link to COVID-19 vaccines, either. In fact, I think I’ll just post this, which includes Sen. Johnson’s letter to the Secretary of Defense, which has gone viral on all social media platforms:
The specific claims that were made by Renz and his “whistleblowers” include that, since the COVID-19 vaccines have rolled out, there have been increases in these conditions:
- Hypertension – 2,181% increase
- Diseases of the nervous system – 1,048% increase
- Malignant neoplasms of esophagus – 894% increase
- Multiple sclerosis – 680% increase
- Malignant neoplasms of digestive organs – 624% increase
- Guillain-Barré syndrome – 551% increase
- Breast cancer – 487% increase
- Demyelinating – 487% increase
- Malignant neoplasms of thyroid and other endocrine glands – 474% increase
- Female infertility – 472% increase
- Pulmonary embolism – 468% increase
- Migraines – 452% increase
- Ovarian dysfunction – 437% increase
- Testicular cancer – 369% increase
- Tachycardia – 302% increase
Unsurprisingly, the Renz Law website is touting these numbers and, of course, complete with any “whistleblower” complaint, there has to be a “coverup”:
Renz also informed me that some DMED data showing registered diagnoses of myocarditis had been removed from the database. Following the allegation that DMED data had been doctored, I immediately wrote to you on January 24 requesting that you preserve all records referring, relating, or reported to DMED. I have yet to hear whether you have complied with this request.
Unsurprisingly, this narrative is being promoted by those with a history of promoting antivaccine misinformation, such as Mike Adams, Steve Kirsch, and Dr. Robert Malone, as well as the entire COVID-19 conspiracy theory, antimask, and antivaccine media ecosystem, for example by The Blaze, the narrative being:
Three military doctors have presented queried data to Renz that shows a shocking and sudden spike in nearly every ICD code for common vaccine injuries in 2021.
In a declaration under penalty of perjury that Renz plans to use in federal court, Drs. Samuel Sigoloff, Peter Chambers, and Theresa Long — three military doctors — revealed that there has been a 300% increase in DMED codes registered for miscarriages in the military in 2021 over the five-year average. The five-year average was 1,499 codes for miscarriages per year. During the first 10 months of 2021, it was 4,182. As Renz explained to me in an interview with TheBlaze, these doctors queried the numbers for hundreds of codes from 2016 through 2020 to establish a baseline five-year average. These codes were generally for ailments and injuries that medical literature has established as being potential adverse effects of the vaccines.
Renz told me the numbers tended to be remarkably similar in all those preceding years, including in 2020, which was the first year of the pandemic but before the vaccines were distributed. But then in 2021, the numbers skyrocketed, and the 2021 data doesn’t even include the months of November and December. For example, some public health officials speculate that COVID itself places women at higher risk for miscarriages. But the number of miscarriage codes recorded in 2020 was actually slightly below the five-year average (1,477). However, they were not drastically below the average on any one category in a way that one can suggest it reflects lockdown-related decreases in doctor’s visits, which somehow led to an increase in 2021 diagnoses.
The database has all the ICD codes for both military hospital visits and ambulatory visits. The data presented by Renz so far is all from the query of ambulatory diagnosis data.
Let’s take a look. Some of these claims will be easy to deal with as highly unlikely to be related to vaccines. Others are a bit less obvious, but still likely spurious, particularly when you recall that, unlike VAERS, DMED was never even intended to look for adverse reactions to vaccines and that these “whistleblowers” simply looked at a timeline and assumed, as antivaxxers always do, that whatever changes they observed in the frequency of diagnoses must have been due to the vaccines. Never mind that there had been a pandemic raging for a year before these data.

Here’s a schema from the DMED website illustrating how DMED works.
What is DMED?
Having been unfamiliar with DMED, I had to educate myself regarding what this database is, and it wasn’t hard to find the DoD’s DMED factsheet:
The Armed Forces Health Surveillance Branch’s (AFHSB) Defense Medical Epidemiology Database (DMED) is a web-based tool to remotely query de-identified active component personnel and medical event data contained within the Defense Medical Surveillance System (DMSS). A newly released version of the database provides unprecedented access to tri-service epidemiologic data that allows users to query large amounts of data in a timely and efficient manner.
In brief, DMSS provides a health database for military personnel that is available to DoD physicians and healthcare personnel who wish to use it, with DMED providing remote access to a subset of that data:
DMSS contains up-to-date and historical data on diseases and medical events (e.g., hospitalizations, ambulatory visits, reportable diseases, immunizations, HIV tests, etc.) and longitudinal data relevant to personnel characteristics and deployments for all active and reserve component service members. DMED provides remote access to a subset of data contained within the DMSS (only data on active component service members). The DMED application provides a user-friendly interface through which users may perform queries regarding medical health care, including disease and injury rates and relative burdens of disease, for active component service members.
DMED provides access to four types of data: demographic, hospitalization, ambulatory and reportable events data.
DEMOGRAPHIC DATA include service, gender, age category, race, pay grade, and marital status.
HOSPITALIZATION DATA include information from DoD Medical Treatment Facilities (MTFs) and outsourced (non-DoD) hospitalization healthcare provided to active component service members. For each hospitalization of an active component service member, at the time of discharge, up to eight diagnoses are recorded (using standard diagnostic codes, International Classification of Diseases (ICD) 9th and 10th revision).
AMBULATORY DATA include information from MTFs and outsourced (non-DoD) ambulatory healthcare provided to active component service members. A maximum of four diagnoses using ICD-9 and ICD-10 codes are recorded for each ambulatory visit of an active component service member.
REPORTABLE EVENT DATA contain information on medical events that are required as defined in the Armed Forces Reportable Medical Events Guidelines and Case Definitions. These data are a subset of information provided by the Disease Reporting System Internet (DRSi).
In addition, DMSS uses various data sources:
DMSS is a relational database with multiple sources feeding information into tables containing information related to the health of U.S. Military Service members. These data sources include, but are not limited to: Defense Manpower Data Center (DMDC), Military Entrance Processing Command (MEPCOM), Defense Health Services System (DHSS), Defense Enrollment Eligibility Reporting System (DEERS), Armed Forces Medical Examiner System (AFMES), DRSi, Pharmacy Data Transaction Service (PDTS), Pharmacoeconomic Center (PEC), and Theater Medical Data Store (TMDS). The Armed Forces Health Surveillance Division (AFHSD) uses this system to generate their master line list of COVID-19 cases, which is shared with APHC, USAFSAM, and NMCPHC.
From my reading, DMED, which allows easy access to the subset of deidentified data from DMSS described above, is a rather odd beast, a front end to a larger database that is a hybrid of passive and active reporting systems in the military, such as the DRSi (passive, used for what the military calls “reportable medical events” or RMEs) and hospitalizations, clinic visits, and diagnosis codes (active), restricted only to current active-duty personnel. Also, most RMEs appear to be infectious diseases, as described in the Armed Forces Reportable Medical Events Guidelines and Case Definitions from before the pandemic. Unsurprisingly, though, antivaxxers touting this “whistleblower” describe DMED as the “best epidemiological database in the world.” (It ain’t.)
I’m going to look at the claims of these whistleblowers two ways. First, I’m going to take the observation at face value. Then I’m going to discuss the likelihood of underreporting. The best place to start is with cancer.
Cancer in DMED: A huge red flag for reporting issues
Given that I’m a cancer surgeon and researcher, you might expect that I would immediately focus on the claims about increases in cancer rates since the vaccines rolled out to the military. You’d be right, and this will be where I take the numbers at face value, at least initially. The cancer numbers alone made me seriously question whether there was a problem with the database for two very simple reasons. First, absent other explanations, cancer rates, while they can increase and decrease from year to year, never show incredibly rapid and dramatic changes, such as the increases ranging from 395% (testicular cancer) to 894% (esophageal cancer) reported by the “whistleblowers”. Indeed, the claimed 487% increase in breast cancer from year to year really got my attention, because such an increase can only be accounted for by reporting issues. For example, as I’ve discussed a number of times before, breast cancer has been relatively stable over the last 30 years, as mortality from breast cancer has been steadily falling, trends that continue based on the 2022 cancer statistics reported last month by the American Cancer Society.
That’s why I can’t take these numbers at face value. Even before I learned more, I concluded that something must be wrong with the database. I’ll show you what I mean. Just for comparison, let’s look at the graph for yearly cancer incidence rates from 1975 to 2018:
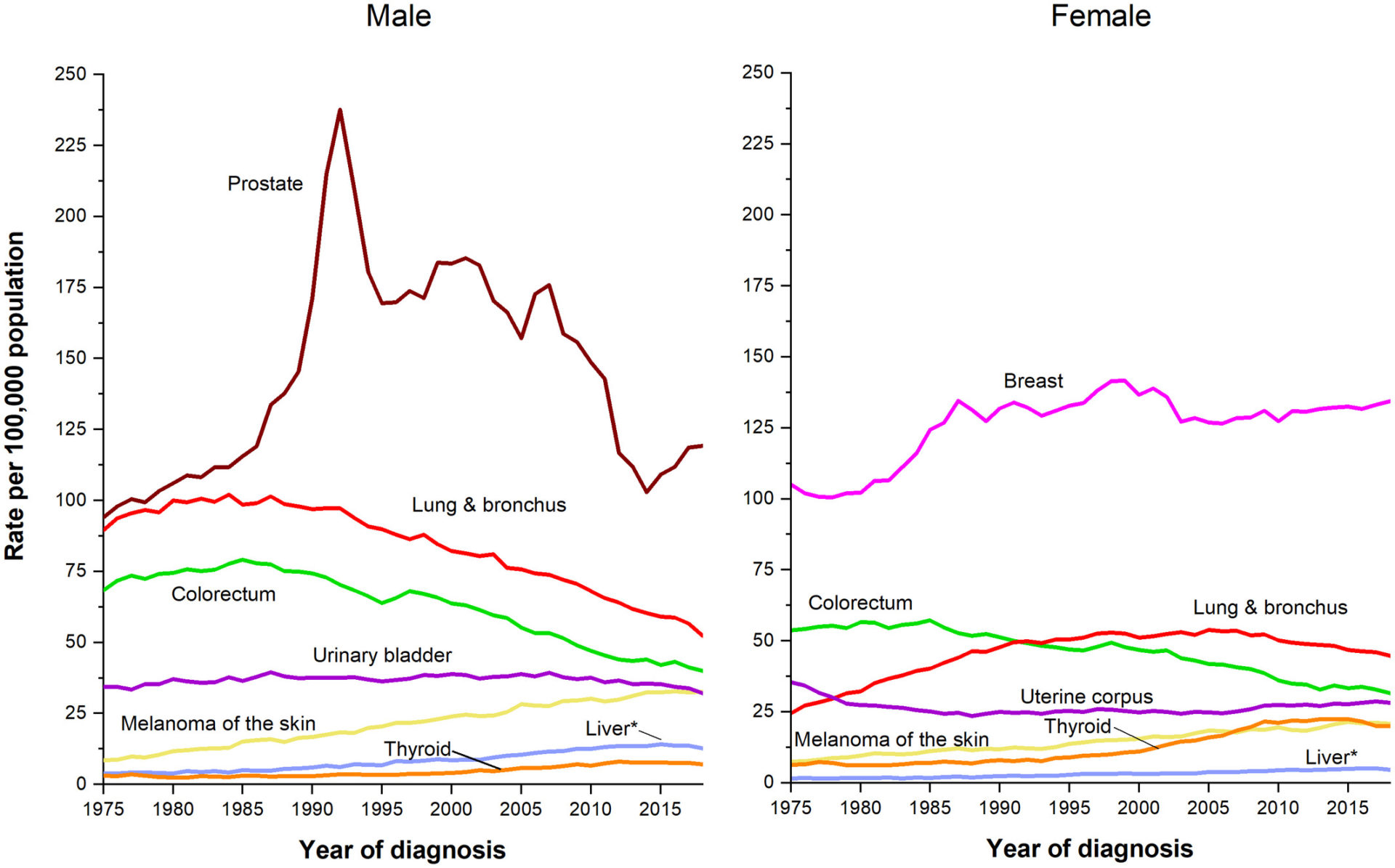
Notice something about these graphs? The very fastest increases in cancer incidence observed are nowhere near what the “whistleblowers'” DMED database dump shows.
Notice that the largest spike in incidence for any cancer was for prostate, a 2.5-fold increase that occurred over 15 years due to the implementation of PSA screening and the overdiagnosis that resulted. Overdiagnosis is the discovery through screening of disease that would never have progressed in a patient’s lifetime to threaten their life, and PSA was great at detecting indolent prostate cancer that either doesn’t progress or progresses so slowly that the patient dies of something else before the cancer spreads.
Spikes in cancer incidence in just one year reported by Renz’s “whistleblowers” are, quite simply, completely implausible from a biologic standpoint. Why is that? Cancer is the culmination of a process that, in general, takes years, from the initial insult that resulted in cellular transformation to the development of a cancerous tumor detectable by symptoms, physical exam, or screening tests. Even if there had been a spike in these cancers from roughly four- to ten-fold in just one year (for an overall increase in total cancer diagnoses from 36,050 to 114,645 from 2020 to 2021), it could not possibly have been due to what Mike Adams, Thomas Renz, and his “whistleblowers” are claiming, namely COVID-19 vaccines, which only started rolling out to the military a year ago and were only mandated for all military personnel after the August 24 order by the Secretary of Defense. Of note, the data from the “whistleblowers” only includes 2021 data through October, with the Army, for instance, not reporting a 98% vaccination rate until mid-December. While those promoting this DMED data dump as smoking gun evidence that COVID-19 vaccines are causing an epidemic of cancer in the military love to point out that the numbers included for 2021 are incomplete, in actuality that incompleteness makes them even more improbable as evidence for COVID-19 vaccines causing cancer, at least. A far more probable explanation is some sort of underreporting in the years prior to 2021.
Alternatively, another potentially plausible explanation is this one:
…a whole bunch more people went to the doctor this year with COVID related issues and also managed to find early cancer diagnoses?
— Teacher and Adjunct Professor (@TurnedLawyer) February 6, 2022
Let’s just put it this way. Say that I was an antivax “whistleblower” who wanted to dumpster dive in a database, say the DMED database, in order to suggest that COVID-19 vaccines cause all sorts of health problems. Let’s say that I was also fortunate enough to come across a situation where there were huge single-year changes in the incidence of a number of diseases, as Renz’s “whistleblowers” were. Knowing cancer as I do, I would have left out the changes in cancer diagnoses, because such huge changes from year to year in cancer diagnoses are so biologically implausible as to bring into question everything else reported. Cancer biologists, doctors, and epidemiologists would immediately recognize that there has to be a reporting issue going on, because such massive increases in cancer incidence in a single year are always due to something like that and not to an environmental exposure, drug, or vaccine, again, because cancer does not develop that fast. If COVID-19 vaccines really did cause cancer, we would not expect to see it for at least a few years; we would not expect to see it in less than a year.
Don’t believe me? Check out this ASCO Post article by Dr. Robert Peter Gale, an oncologist, writing about cancers induced by ionizing radiation:
What do these data show? First, the risk of developing a radiation-induced cancer is dose-related—the higher the dose, the greater the probability a cancer in an A-bomb survivor was caused by radiation exposure. Second, the A-bomb data allow us to determine the briefest interval from radiation exposure to cancer diagnosis. For leukemias, this is about 2 years, and for solid cancers, about 10 years. These increased risks, especially those for solid cancers, were most easily detected after 30 years and remain over a person’s lifetime.
Again, the cancer data reported in the DMED data dump, even leaving aside that there is no correlation shown between COVID-19 vaccination and the diseases attributed to it given that COVID vaccination status was not included in the data downloaded, are the biggest “tell” that something other than a real effect due to COVID-19 vaccines (or anything else) is the explanation for such massive increases in cancer incidence in just one year. To believe that COVID-19 vaccines were responsible for this increase in cancer incidence among military personnel, one would be obligated to believe that COVID-19 vaccines are far more carcinogenic than ionizing radiation from atomic bombs. After all, the DMED data revealed increases in the incidence of solid tumors like esophageal and other GI cancers that were reported less than a year after the vaccines became available. Come to think of it, I didn’t see any mention of hematologic malignancies, like leukemias in this “whistleblower” report. Odd, isn’t it? The cancers that are known to appear the fastest after exposure to a powerful carcinogen like ionizing radiation don’t show up as having increased in incidence in this report. One wonders if there were some cherry picking, one does. After all, I’m sure that the data for hematologic malignancies must be in DMED. Why didn’t the “whistleblowers” download the data? Or maybe they did, and Renz left it off the Excel spreadsheet because was no change in incidence from 2020-2021.
Fortunately, like Dr. Ryan Cole before them (who also tried to link COVID-19 vaccines to increased cancer diagnoses while neglecting cancer biology and as a pathologist really should have known better), neither Renz nor Drs. Sigoloff, Chambers, and Long were smart enough to realize that the cancer numbers alone are huge red flags that something other than the COVID-19 vaccines likely explain the single year increases in all of these conditions. Even Dr. Robert “inventor of mRNA vaccines” Malone, who has gone full antivaccine lately, managed to ignore the extreme implausibility of attributing such a huge increase in cancers to COVID-19 vaccine mandates in the military, writing over the weekend:
Notably, we now have Dr. Pierre Kory warning about censoring of early COVID treatment options, and Dr. Ryan Cole raising alarms about an alarming trends in cancer diagnoses which coincide with the onset of mass COVID-19 genetic vaccination.
So, are there any large data sets supporting Dr. Cole’s concerns about cancer incidence, or for that matter my warning to parents about potential genetic vaccine-associated risks to brain, nervous system, heart, immune system, and reproductive systems in children and healthy young adults? Judging by the amount of invective and targeted character assassination attacks which Pierre, Ryan and I have had to endure, we must be raising completely unfounded concerns and spreading disinformation.
Actually, they all have been doing just that, spreading misinformation, but let’s move on.
Here’s the funny thing. Elsewhere in that same recent post, Dr. Malone wrote something that was—for him, at least—shockingly reasonable, in which he cautioned his readers:
Now these are basically raw data from the Defense Medical Epidemiological Database (DMED). For the detail oriented, this is the scrubbed and de-identified (HIPAA compliant) database derived from the Defense Medical Surveillance System (DMSS), which pulls directly from patient records and other US Department of Defense-related medical record information streams. These data were pulled with full chain-of-custody documentation based on various CPT codes that are related to known genetic COVID-19 vaccine side effects.
As raw data, this information needs to be reviewed with care and considered to be both rough and preliminary. For the uninitiated, there are major risks associated with reliance on large, raw (uncorrected) data sets for retrospective (backwards in time) data analyses. The key technical term here is “confounding variables“, but data entry errors (such as multiple entries for the same diagnostic event) or process changes can also introduce huge sources of bias into large data sets like this. With raw data, it is most useful to consider any data plotting to be sort of a first draft, useful for identifying potential trends or topics that deserve more detailed analysis.
Unfortunately, Dr. Malone couldn’t restrain himself from continuing:
But sometimes, when the observed effect size in the raw data is very large or potentially important, alarm bells start ringing even before full analysis is completed. And that seems to be the case with these data.
Actually, when the effect size is so huge as to be incredibly implausible from a biological standpoint, as the reported DMED data for overall cancer rates and the increases in various specific cancers reported are, such enormous observed effect sizes do cause alarm bells to start ringing, just not for the reasons that Dr. Malone cites. In such a case, alarm bells ring because there’s very likely something “off” or wrong with the dataset and suggest that the observed effect size is due to issues with reporting, rather than a real change in incidence rates.
Amusingly, Dr. Malone cites an observation from another antivaccine doctor that an “instructive test would be to check that we do not see a similar rise for conditions that could not plausibly exhibit a significant association with the vaccines, such as broken legs or burns.” Funny, isn’t it, that Renz’s “whistleblowers” didn’t do even that simple quality test. Come to think of it, why doesn’t Dr. Malone insist that they do this simple test?
If you are so inclined, you too can download the Excel spreadsheet from the Renz Law website. Interestingly, none of the conditions for which the “whistleblowers” downloaded data is a condition like the ones suggested by Dr. Malone as useful to look at as negative controls, and all of the conditions included show massive increases in incidence, which leads me to suspect cherry picking. In any event, as soon as I saw the one-year increases in cancer incidence ranging from 300% to nearly 1,000%, I knew that the explanation had to be either a reporting problem, the DMSS database itself or how it pulls data from the various other databases that feed it, or a bug in the algorithm by which DMED pulls data from the DMSS database in queries—had to be. The true incidence of cancer doesn’t increase so dramatically in less than a year. It had to be underreporting in years before or a bug in how data were pulled over to DMED. A cardinal rule of evaluating results of a database search is that if some of the results are clearly impossible, then you have to assume that the problem is with the database or the algorithm, not that the impossible results are real. Of course, Renz, being an antivax lawyer looking to make a name for himself bringing various dubious lawsuits against vaccine mandates and representing these “whistleblowers,” assumed the clearly highly implausible data were real and, as antivaxxers always do, assumed that the COVID-19 vaccines were the explanation. The “whistleblowing” doctors should have known better, at least about the cancer rates—no, seriously, people, how could you not have realized the utter implausibility of these results?—but I can only assume that they are antivax too.
The “coverup”
In the world of antivaccine conspiracy theories, there must always be some sort of “coverup”. All conspiracy theories involve a “coverup”, particularly antivaccine conspiracy theories. For example, the Simpsonwood conspiracy theory that claimed that the CDC met in 2000 to “cover up” and “massage” data showing that thimerosal in childhood vaccines had resulted in a massive increase in the prevalence of autism, and the “CDC whistleblower” conspiracy theory behind the antivaccine propaganda film disguised as a documentary VAXXED postulated a CDC coverup of data showing that the MMR vaccine had resulted in a four-fold increase in autism among African-American boys. So it is with this conspiracy theory as well, with Steve Kirsch gloating:
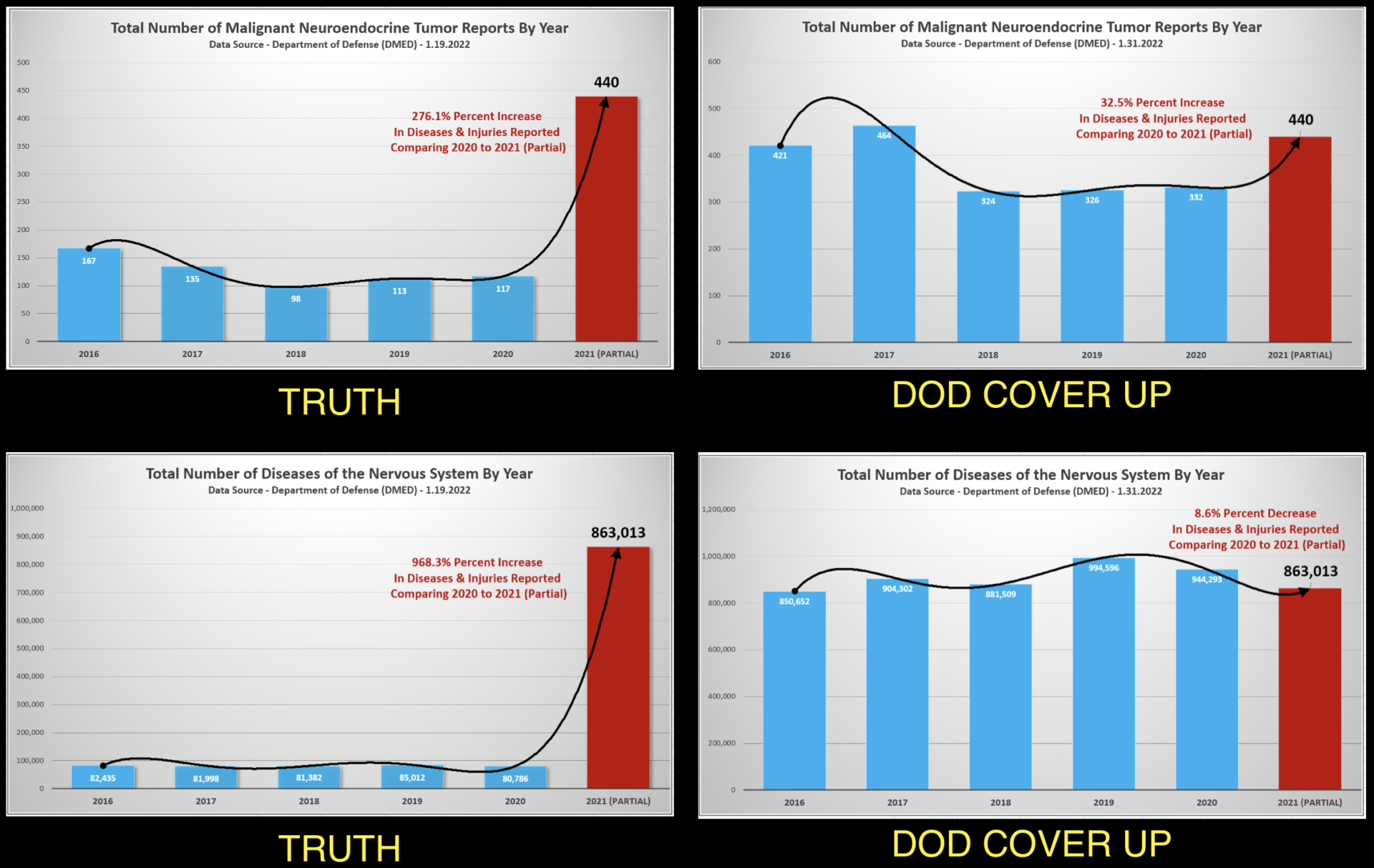
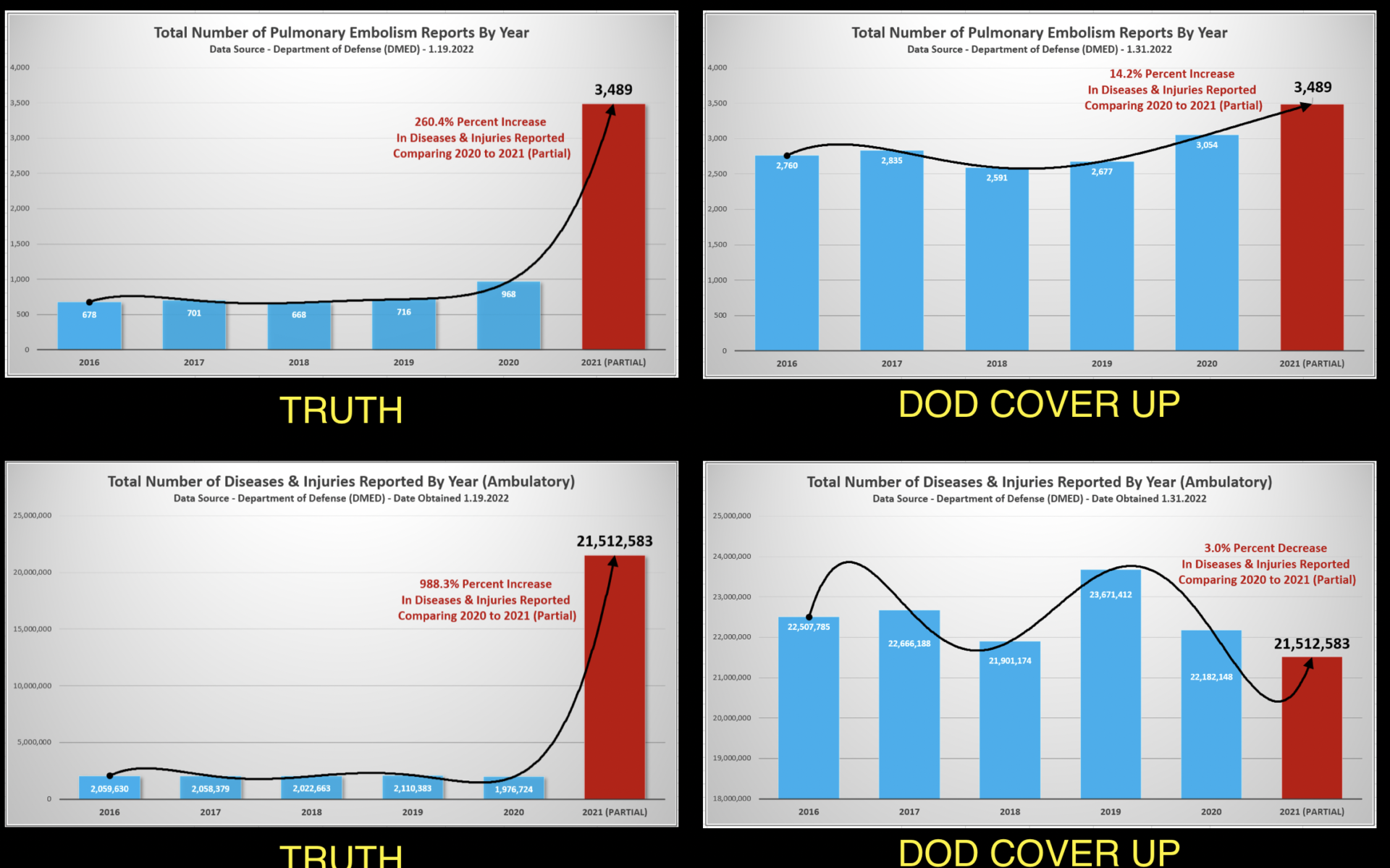
The original DMED data appears to be very reliable. It is hard for anyone to make excuses for the increased rates in the DMED database quoted in this letter because the event types with increases are all confirmed in the VAERS database. Unlike VAERS, this database cannot be dismissed using hand-waving arguments. DMED is not a self-reported database where reporting rates are unknown. It is a fully reported database where all the reports are from healthcare providers. In short, if the vaccines are safe, the DMED data is hard to explain. For example, you can’t pin the rise in events in 2021 on COVID since total hospital event rates declined in 2020 (relative to 2019) in both the original and corrected results. Note: The DoD now claims the 2016-2020 data was wrong and issued corrected values (graph on the right):
And here’s the figure:
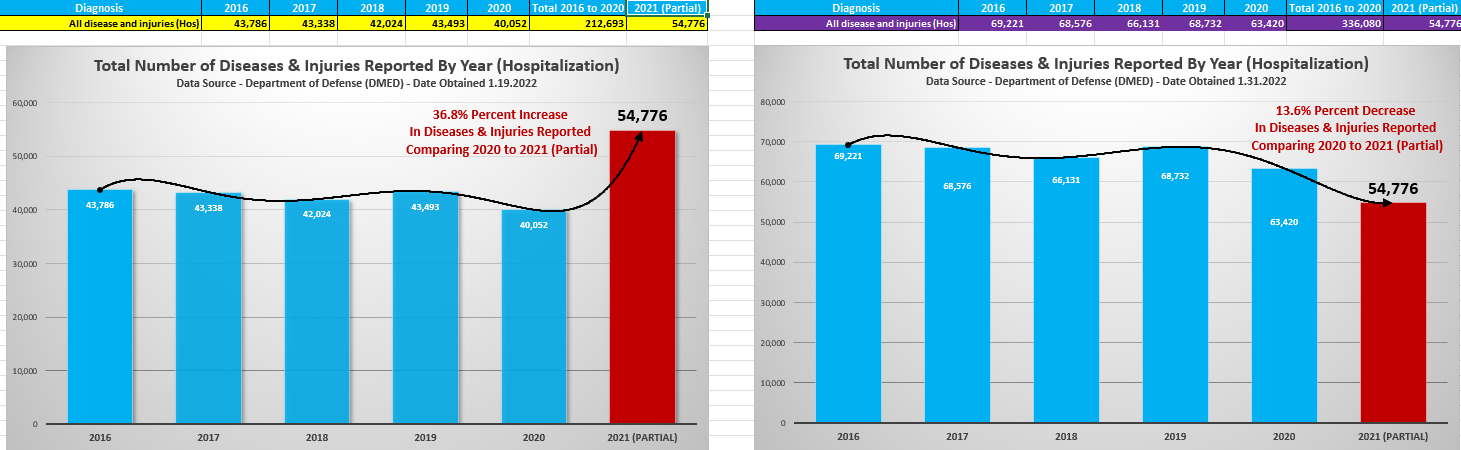
DMED data: Before and after correction.
The Renz Law Firm goes even further, predictably, as these screenshots of its website yesterday show:
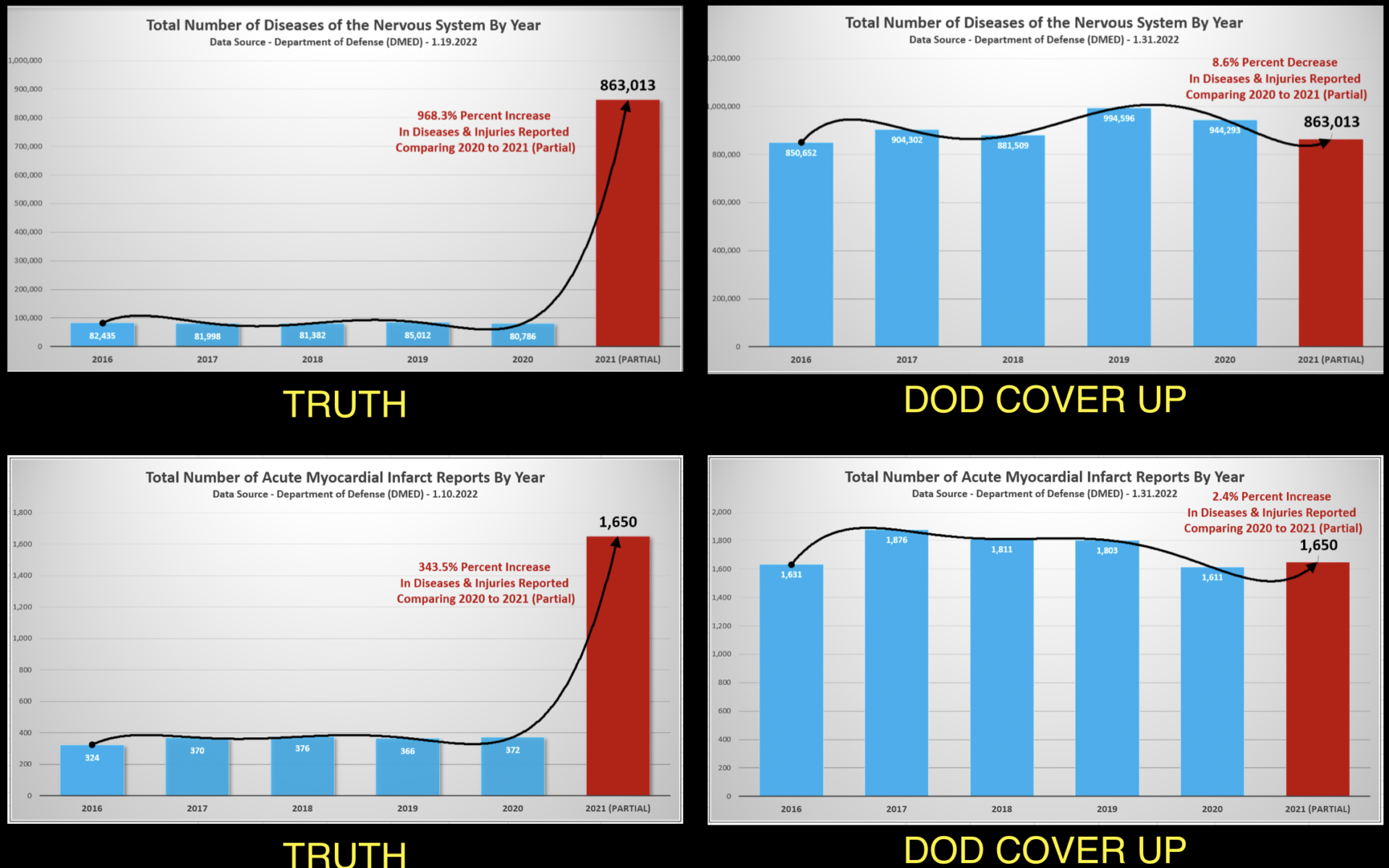
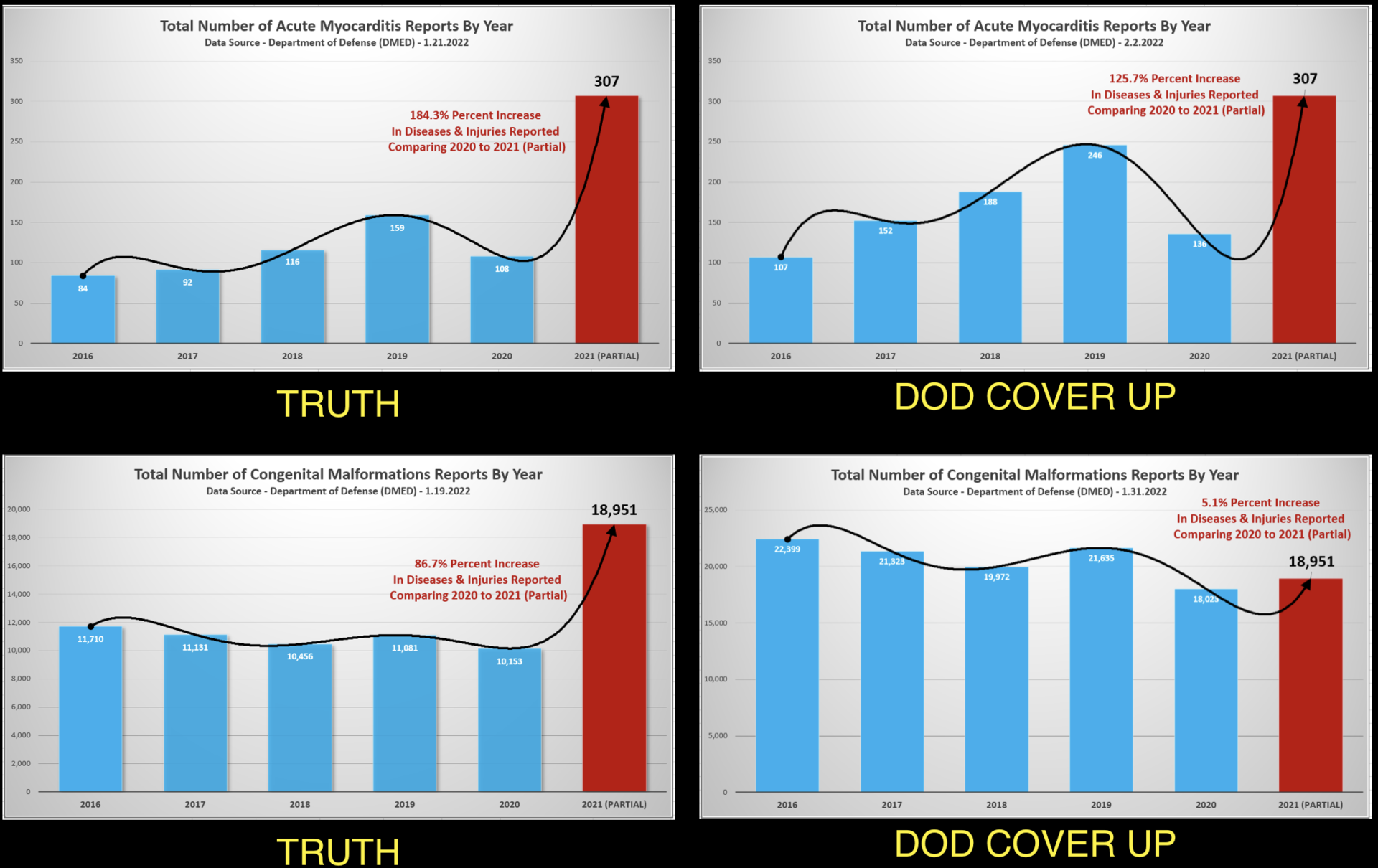
DMED “coverup”? I sense a…theme…here.
And then Kirsch goes on:
The DoD is in a panic about this leaking out. This data wasn’t ever supposed to leak out. The only reason it leaked out is due to the efforts of three whistleblowers inside the DoD. According to an insider I spoke to, the DoD has no idea how they are going to cover it up. The only thing they’ve done is claim the 2016-2020 data is underreported, but this doesn’t match reality as I explain below.
And, of course, the mainstream press is also in on the “coverup”:
Deliberate mainstream press cover-up. There is evidence that mainstream media reporters have been instructed not to cover this story or talk to Tom Renz. I verified this myself searching for articles about Renz in The New York Times and CNN. So you’ll only hear about it from alternative media. Think about it… this is one of the most explosive stories of the year (if not the decade) and the mainstream press isn’t covering it at all? What does that tell you? You don’t have to have a lot of critical thinking skills to figure that one out. It pretty much tells you everything you need to know: there is a massive cover up of adverse events.
And even these enormous increases are an “underestimate” of the true numbers, because of course they are:
It’s important to note that the soldiers are tough and don’t want anything on their medical records that could limit their responsibilities
The coverup is of course why, if you look at the actual Excel spreadsheet, you will see corrected numbers added, and, of course, to Kirsch it’s obviously a plot by the DoD to “cover up” the “injuries” from COVID-19 vaccines in the military. The amusing thing to me, though, is that, even though I don’t trust the military to be truthful any more than anyone else, from a biological, scientific, epidemiological, and medical perspective, underreporting during previous years is in actuality a far more plausible explanation for what is seen in the data downloaded by these “whistleblowers” and now being weaponized by antivaccine lawyers and propagandists than is a real increase in incidence of all these medical conditions due to COVID-19 vaccines.
The “coverup” then proceeds to get even worse and more egregious, with an article published by Politifact, which deemed the “whistleblower” claims to be false:
But Peter Graves, spokesperson for the Defense Health Agency’s Armed Forces Surveillance Division, told PolitiFact by email that “in response to concerns mentioned in news reports” the division reviewed data in the DMED “and found that the data was incorrect for the years 2016-2020.”
Officials compared numbers in the DMED with source data in the DMSS and found that the total number of medical diagnoses from those years “represented only a small fraction of actual medical diagnoses.” The 2021 numbers, however, were up-to-date, giving the “appearance of significant increased occurrence of all medical diagnoses in 2021 because of the underreported data for 2016-2020,” Graves said.
The DMED system has been taken offline to “identify and correct the root-cause of the data corruption,” Graves said.
Remember, DMED is more or less a subset of the DMSS in which the data have been deidentified; so it is the data in the DMSS that would be the complete dataset, not what’s seen in the DMED. That being said, it is rather disturbing that before 2021 there had apparently been some sort of problem with DMED such that what it pulled from the DMSS was only a fraction of the medical diagnoses there, but somehow whatever glitch caused that underreporting was fixed by 2021 but not for the years before. It’s an unforced error that was custom-made for conspiracy theorists and will likely make it impossible to convince many people that these data were full of underreporting before 2021, even though the cancer rates found were a huge red flag that something like this must have been occurring, leading Dr. Malone to opine:
Now for some reason, although this database has apparently been managed for years by the same NIH subcontractor, and has been included in the CDC datasets including those reviewed by the CDC’s COVID-19 Vaccine Safety Technical (VaST) Work Group, the geniuses that have been managing it have never identified any issues before the whistleblowers grabbed this download. Does not inspire confidence, no matter what the final “official” explanation becomes.
Unfortunately, a lot of people will find the seeming conspiracy to “cover up” the findings of the “whistleblowers” compelling. Truly, at best this was an unforced error on the part of the DoD.
A teachable moment
I can’t resist relating this DMED kerfuffle back to the primary mission of SBM. Longtime readers will recall that the founders of this blog originally proposed the idea that alternative medicine claims—indeed all medical claims—need to be considered through the lens of prior biological plausibility. That’s why, for example, we can dismiss homeopathy as impossible based on basic science considerations along, regardless of what bias- and error-prone clinical trials show. After all, as we have long pointed out, for homeopathy to be true, not only would huge swaths of what we know about physics, chemistry, and biochemistry have to be wrong, they’d have to be spectacularly wrong. While it is possible (just barely) for this to be true, it is up to homeopathy advocates to provide scientific evidence of sufficient quality and quantity to overthrow all the principles of physics and chemistry that homeopathy violates, not up to scientists to “prove them wrong”.
We can apply the same principle to the DMED data dump, which is marginally only somewhat less implausible than homeopathy. For the observed increases in cancer incidence reported by these feckless “whistleblowers” to be true increases, then not only would what huge swaths of what we know about cancer and carcinogenesis have to be wrong, but they’d have to be spectacularly wrong. You can safely ignore everything else reported in the data dump for the simple reason that what’s reported for cancer is so incredibly implausible that it has to be due to reporting error. That was true before the DoD issued that statement to Politifact and took the DMED offline to investigate, and it’s even more true now.
Add to that the fact that the man orchestrating the “whistleblower” report is a lawyer with a long history of suing for “vaccine injury” and promoting antivaccine misinformation and who filed a lawsuit on behalf of the COVID-19 minimizing group America’s Frontline Doctors alleging that the “true” number of deaths due to the COVID-19 vaccines is being “covered up” and has a history of misusing other databases to misleadingly claim that COVID-19 vaccines are causing tens of thousands of deaths, and you can be quite confident that the claims of these whistleblowers are not supported by any actual science or epidemiological evidence. This is doubly true given that the “whistleblowers” didn’t bother to do checks on their data so simple that even an antivaccine crank like Dr. Robert Malone recognized that they were important.
Thus endeth this week’s teachable moment. I fear that it won’t register among those who most need it.